

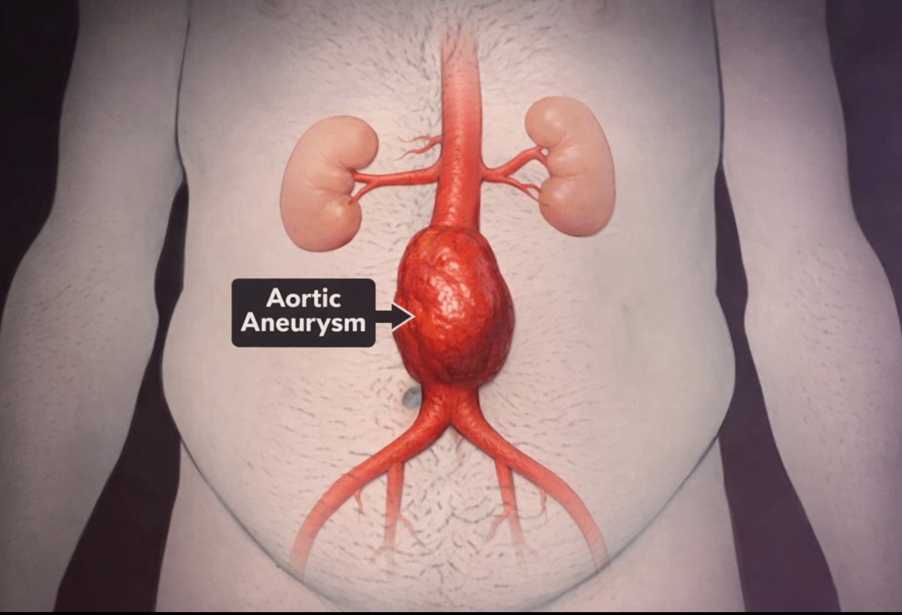
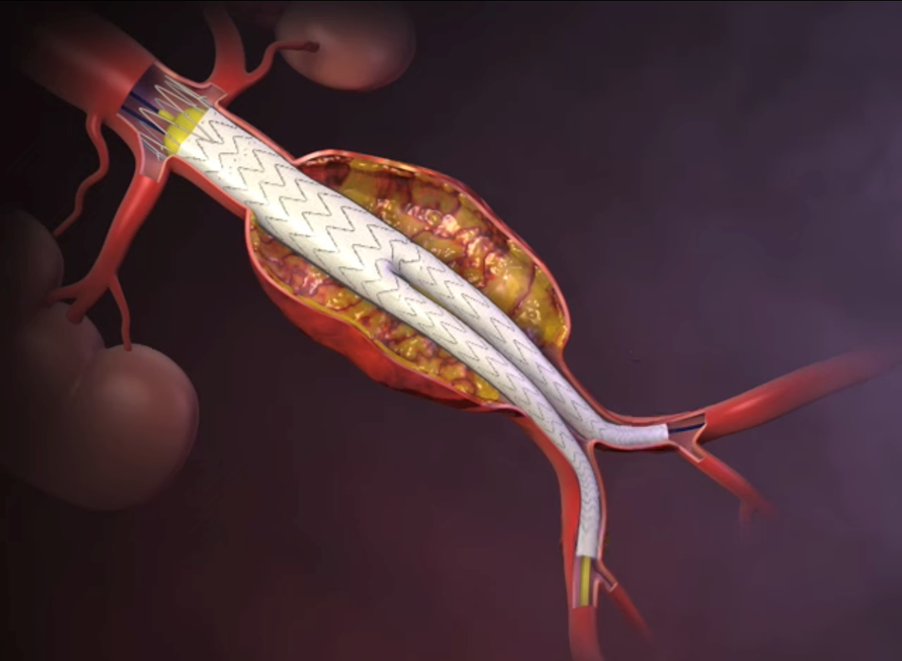
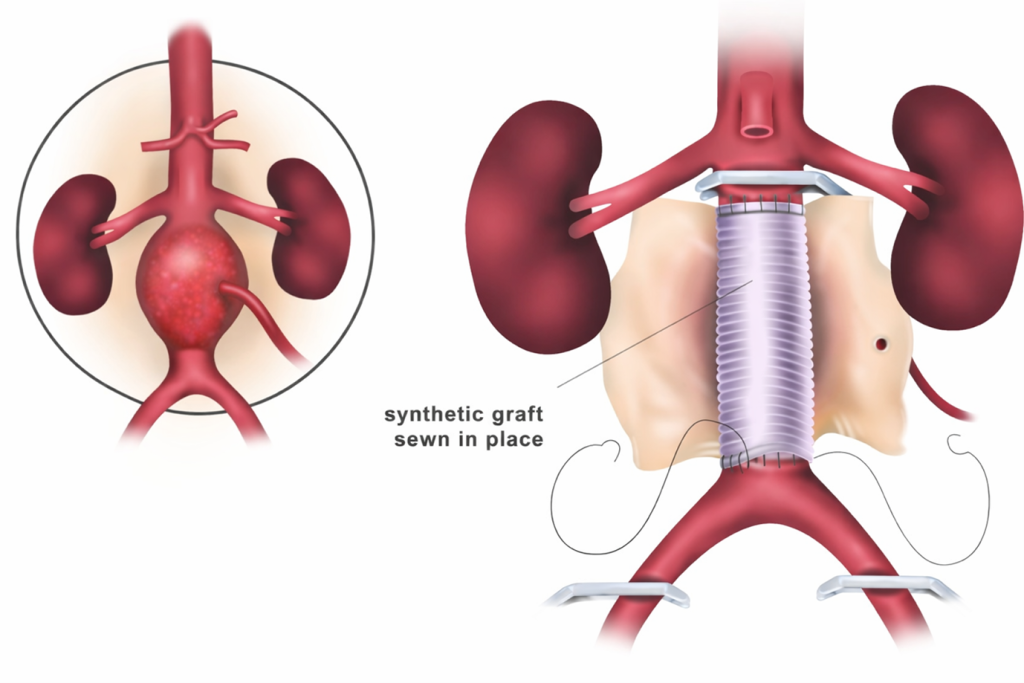
An abdominal aortic aneurysm (AAA) happens when the lower part of your body’s main artery — the aorta — becomes enlarged. The aorta runs from your heart, through your chest, and into your abdomen.
AAAs usually grow slowly. In most cases, you will not notice any symptoms, which is why they are often discovered incidentally or through screening. Some aneurysms remain small and stable. Others enlarge over time, sometimes quickly. If an aneurysm ruptures, it can cause life-threatening internal bleeding.
What symptoms might you notice?
If your aneurysm is enlarging, you may experience:
- Deep, constant pain in your abdomen or the side of your abdomen
- Persistent back pain
- A throbbing or pulsing sensation near your belly button
If an aneurysm ruptures, symptoms can include:
- Sudden, severe and persistent abdominal or back pain (often described as tearing or ripping)
- Dizziness or fainting due to low blood pressure
- A rapid pulse
A ruptured aneurysm is a medical emergency and requires immediate treatment.
What increases your risk?
You are more likely to develop an abdominal aortic aneurysm if you:
- Smoke or have smoked– this is the strongest risk factor. Smoking weakens the aortic wall and increases the risk of growth and rupture.
- Are aged 65 or older
- Are male
- Have a family history of abdominal aortic aneurysm
- Have had another aneurysm (for example in the chest or behind the knee)
- Have high blood pressure or other cardiovascular disease
How can you reduce your risk?
You can lower your risk of developing or worsening an aneurysm by:
- Stopping smoking and avoiding second-hand smoke
- Controlling your blood pressure and cholesterol
- Eating a balanced diet rich in fruit, vegetables, whole grains and lean protein
- Reducing salt and unhealthy fats
- Exercising regularly (aim for at least 150 minutes of moderate activity per week, if appropriate for you)
NHS AAA Screening Programme (NAAASP)
If you are a man aged 65 or over in England, you will automatically be invited for a free abdominal aortic aneurysm screening scan through the NHS Abdominal Aortic Aneurysm Screening Programme.
This involves a quick, painless ultrasound scan of your abdomen to check the size of your aorta.

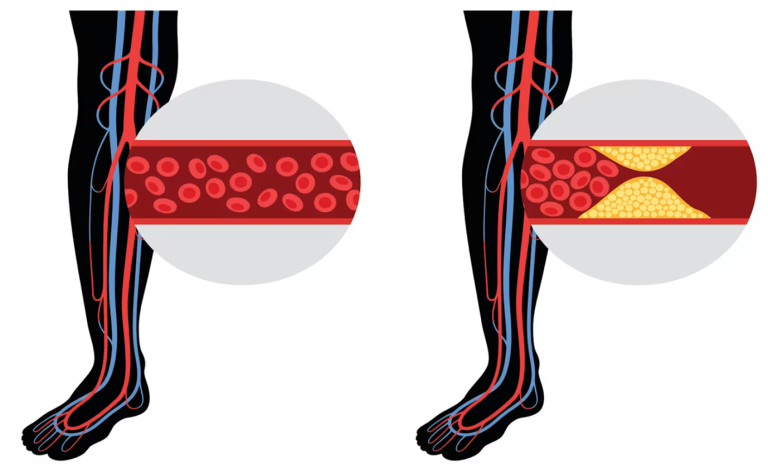
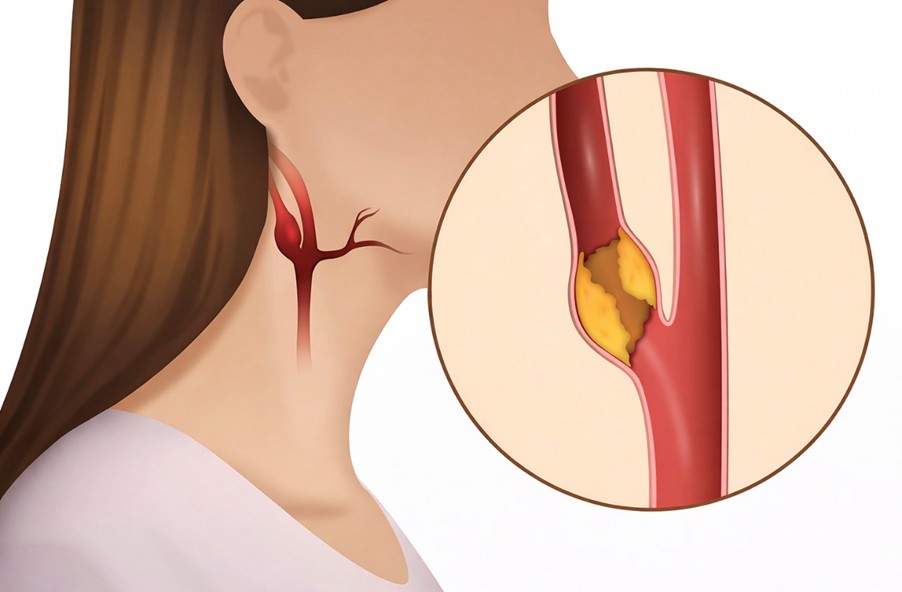
Carotid artery disease develops when fatty deposits (plaques) build up inside the arteries in your neck that supply blood to your brain. These arteries are called the carotid arteries.
When they become narrowed or blocked, your risk of stroke increases significantly.
A stroke is a medical emergency. It happens when part of your brain loses its blood supply. Without oxygen, brain cells begin to die within minutes, which can lead to permanent disability or death.
Carotid artery disease usually develops slowly. In many cases, the first warning sign may be a transient ischaemic attack (TIA) or a stroke.
A TIA is a temporary interruption of blood flow to your brain. Symptoms resolve completely, but it is a serious warning that you are at high risk of a full stroke.
Symptoms
In the early stages, you may have no symptoms at all. Symptoms usually appear when blood flow to your brain becomes critically reduced.
Signs of a stroke or TIA include:
- Sudden numbness or weakness in your face, arm or leg — often on one side.
- Sudden difficulty speaking or understanding speech.
- Sudden loss of vision in one or both eyes.
- Sudden dizziness, unsteadiness or loss of balance.
- Sudden severe headache with no obvious cause.
When to Seek Medical Help
If you develop any symptoms of a stroke — even if they last only a few minutes — seek emergency medical care immediately.
Do not ignore temporary symptoms. A TIA is a warning sign that you are at high risk of a major stroke.
If you have risk factors for carotid artery disease, you should consider vascular assessment even if you feel well. Early detection significantly reduces your stroke risk.
Causes
Carotid artery disease is caused by atherosclerosis — the gradual build-up of cholesterol, fat, and inflammatory cells inside your artery walls.
As plaque accumulates:
- Your carotid arteries become narrowed.
- Blood flow to your brain is reduced.
- Oxygen and nutrients cannot reach brain tissue adequately.
Risk Factors
You are at higher risk if you:
- Have high blood pressure.
- Smoke or use tobacco.
- Have diabetes.
- Have high cholesterol or high triglycerides.
- Have a family history of atherosclerosis or heart disease.
- Are older.
- Are overweight or obese.
- Have sleep apnoea.
- Do not exercise regularly.
Many of these risk factors are treatable. Controlling them significantly reduces your stroke risk.
How Carotid Artery Disease Causes Stroke
Carotid artery disease is responsible for approximately 10% of strokes. Stroke can occur in several ways:
1. Severely Reduced Blood Flow
Your artery may become so narrowed that insufficient blood reaches part of your brain.
2. Plaque Rupture
A fragment of plaque can break off and travel to smaller brain arteries, blocking blood flow.
3. Blood Clot Formation
Plaques can crack, triggering clot formation. A clot may grow large enough to block the artery or travel to the brain.
All three mechanisms can suddenly stop blood supply to part of your brain.
Protecting Yourself
Early diagnosis and treatment can prevent stroke. Management may include:
- Strict blood pressure control
- Cholesterol-lowering medication
- Antiplatelet therapy
- Lifestyle modification
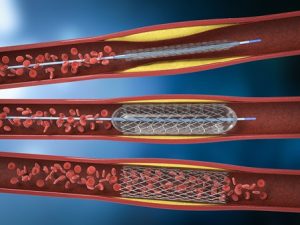
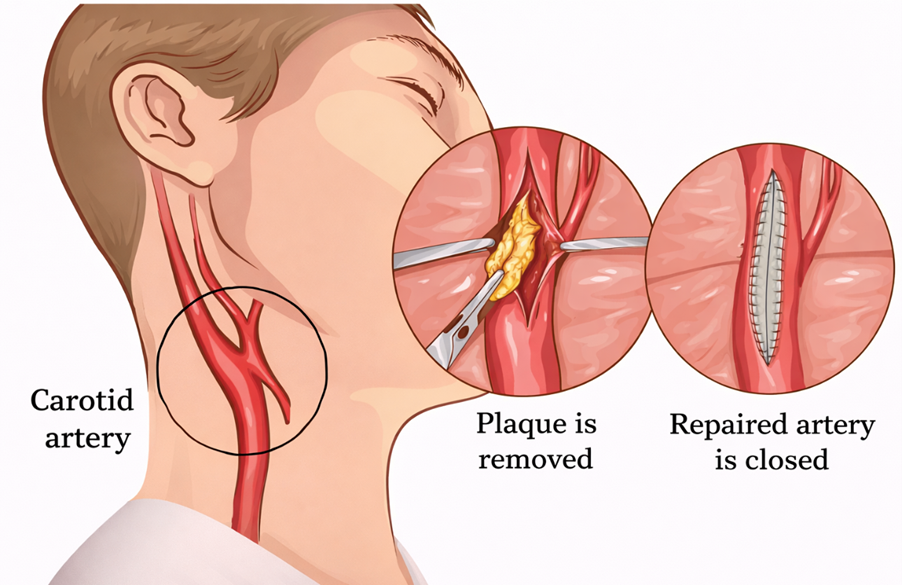
- Carotid endarterectomy or carotid stenting in selected patients
If you have experienced a TIA, stroke symptoms, or have multiple vascular risk factors, specialist assessment is essential.
Diagnosis of Carotid Artery Disease
Your assessment usually begins with a detailed medical history and physical examination.
During the examination, your neck will be checked with a stethoscope to listen for a “bruit” — a whooshing sound caused by turbulent blood flow in a narrowed carotid artery.
You may also undergo a brief neurological assessment to check your:
- Strength
- Speech
- Memory
- Coordination
These tests help determine whether your brain circulation has already been affected.

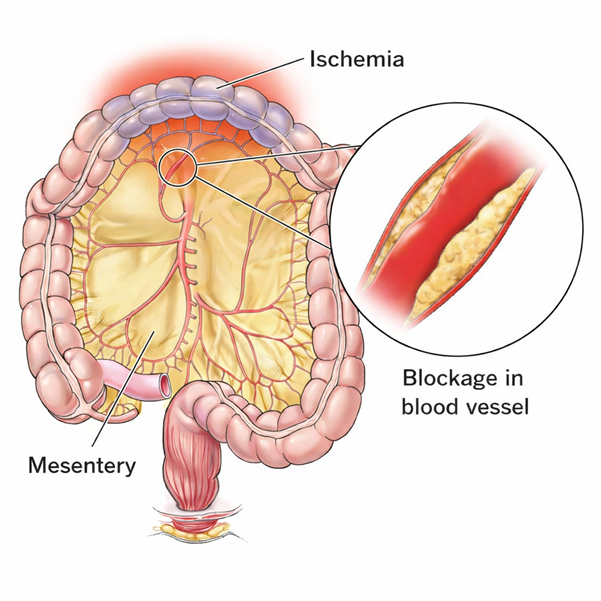
Mesenteric ischaemia occurs when the arteries supplying your small intestine become narrowed or blocked, reducing blood flow. If untreated, the reduced circulation can permanently damage your intestine.
When this problem develops gradually over time, it is called chronic mesenteric ischaemia. It is usually caused by a build-up of fatty deposits (atherosclerosis) within the mesenteric arteries (arteries that supply your bowel)
If left untreated, the chronic form can suddenly worsen and become an emergency (acute mesenteric ischaemia). It can also lead to severe weight loss and malnutrition.
Symptoms You Should Not Ignore
You may experience:
- Abdominal pain starting about30 minutes after eating.
- Pain that gradually worsens over the next hour.
- Progressivefear of eating.
- Unintentional weight loss.
If you develop sudden, severe, persistent abdominal pain, seek urgent emergency care.
If you notice repeated pain after meals, you should arrange specialist vascular assessment without delay.
Why It Happens
Your small bowel relies on three main arteries for blood supply. When these arteries narrow due to plaque build-up, blood flow becomes insufficient — particularly after meals, when your bowel needs more oxygen.
Chronic mesenteric ischaemia is most often caused by:
- Atherosclerosis (fatty plaque narrowing the arteries)
Acute mesenteric ischaemia may occur due to:
- A blood clot (often originating from the heart)
- Sudden blockage of a mesenteric artery (artery supply your bowel)
Risk Factors
You are at higher risk if you have:
- Type 2 diabetes
- High blood pressure
- High cholesterol
- Smoking history
- Obesity
- Known vascular disease
- Atrial fibrillation
- Heart failure
Potential Complications
Without treatment, you may develop:
- Severe weight loss
- Malnutrition
- Acute-on-chronic mesenteric ischaemia (a life-threatening emergency)
Early diagnosis prevents irreversible bowel damage.
When to Seek Specialist Review
If you have:
- Post-meal abdominal pain
- Unexplained weight loss
- Known vascular disease with new abdominal symptoms
You should not delay assessment. Chronic mesenteric ischaemia is treatable — but timing is critical.
Early intervention can restore blood flow, relieve pain, and prevent life-threatening complications.
Diagnosis of Chronic Mesenteric Ischaemia
If you develop abdominal pain after eating and begin limiting your food intake or losing weight unintentionally, this raises concern for chronic mesenteric ischaemia.
The diagnosis is confirmed by demonstrating narrowing or blockage in the main arteries supplying your small bowel.
At Sharkawy Vascular Clinic, you will undergo a structured vascular assessment and advanced imaging techniques to accurately define the severity and anatomical pattern of disease.
Investigations You May Require
1. Doppler Ultrasound
This non-invasive test assesses blood flow velocity in the mesenteric arteries. It is useful for:
- Initial screening
- Follow-up after treatment.
2. CT Angiography (CTA) or MR Angiography (MRA)
These specialised scans provide detailed images of your bowel arteries.
A contrast dye is injected into a vein to make the arteries clearly visible.
All imaging is carefully reviewed to determine:
- Degree of stenosis
- Number of vessels involved
- Suitability for key-hole versus open intervention
When to Seek Specialist Assessment
Arrange urgent review if you have:
- Recurrent abdominal pain after eating
- Unexplained weight loss
- Known vascular disease with new abdominal symptoms
Chronic mesenteric ischaemia is treatable. Early specialist intervention prevents progression to acute intestinal infarction and avoids irreversible bowel damage.
Treatment of Mesenteric Ischaemia
At Sharkawy Vascular Clinic, treatment options include:
1. Endovascular Revascularisation (Minimally Invasive)
- Balloon angioplasty to open the narrowed artery
- Stent placement to maintain patency
- Performed through a small arterial puncture
This approach offers:
- Shorter recovery time
- Reduced surgical trauma
- Effective symptom relief in appropriate cases
2. Open Surgical Revascularisation
For complex disease, open bypass surgery may provide more durable long-term results.
This involves:
- Creating a bypass graft to restore blood flow
- Direct arterial reconstruction when required
My Approach to Your Care
As a Consultant Vascular & Endovascular Surgeon, I provide:
- Comprehensive diagnostic evaluation
- Individualised treatment planning
- Expertise in both open and advanced endovascular techniques
- Care tailored to complex multi-vessel mesenteric disease
You will receive a treatment strategy based on your anatomy, symptom severity, co-morbidities, and long-term durability.

